Maj Smith, a 22-year-old male, was just three weeks into his second tour of duty. While on foot patrol one afternoon, Smith and his squad broke off from the company to begin house-to-house searches in one of the more dangerous neighborhoods in the area. Moments after entering one home, they surprised a group of insurgents, who quickly open fire on the squad.
“I remember ordering my men to take cover and the next thing I knew, I was in a battalion aid station,” recalled Smith.
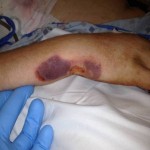
Smith suffered multiple gunshot wounds while trying to get his squad to safety. A nearby squad heard the gunfire and was soon able to contain the insurgents and transport Smith and his men to medical care. Both of Smith’s arms were wounded and he was bleeding from his flank, where a bullet penetrated both his right arm and his chest. Also, he was having difficulty breathing. The company had been well trained in front-line first aid and buddy care. One soldier applied tourniquets to both upper arms to slow the bleeding while another applied direct pressure and clean bandages to Smith’s open wounds. They also performed decompression of Smith’s right chest, which eased his breathing while they waited for the medevac chopper to arrive.
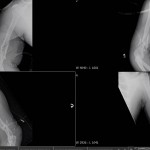
At a nearby combat support hospital, Smith saw the first doctor to manage his many wounds. The diagnosis included orthopaedic injuries consisting of bilateral distal third, open, comminuted humerus fractures, a left small finger comminuted metacarpal fracture, and multiple soft tissue fragmentary injuries. Non-orthopaedic injuries were a right-side pneumothorax, bilateral testicular rupture, and a gunshot wound to the abdomen.
In an echelon 2 medical facility, where basic surgical stabilization care can be provided, what sequence of care would you recommend for this patient?